
In our previous article, we explained Value-Based Care Plans (VBC – aka Capitation) and presented the official policy of the American Dental Association (ADA) against such plans.
Yet just inside the ADA, a powerful group known as the “Dental Quality Alliance” (DQA) is promoting value-based care.
This ADA group has become a VBC platform for dental insurers – who pay for DQA voting rights.
This article is meant to shine a light on this conflict of interest.
BACKGROUND: 2009 FORMATION OF THE DENTAL QUALITY ALLIANCE
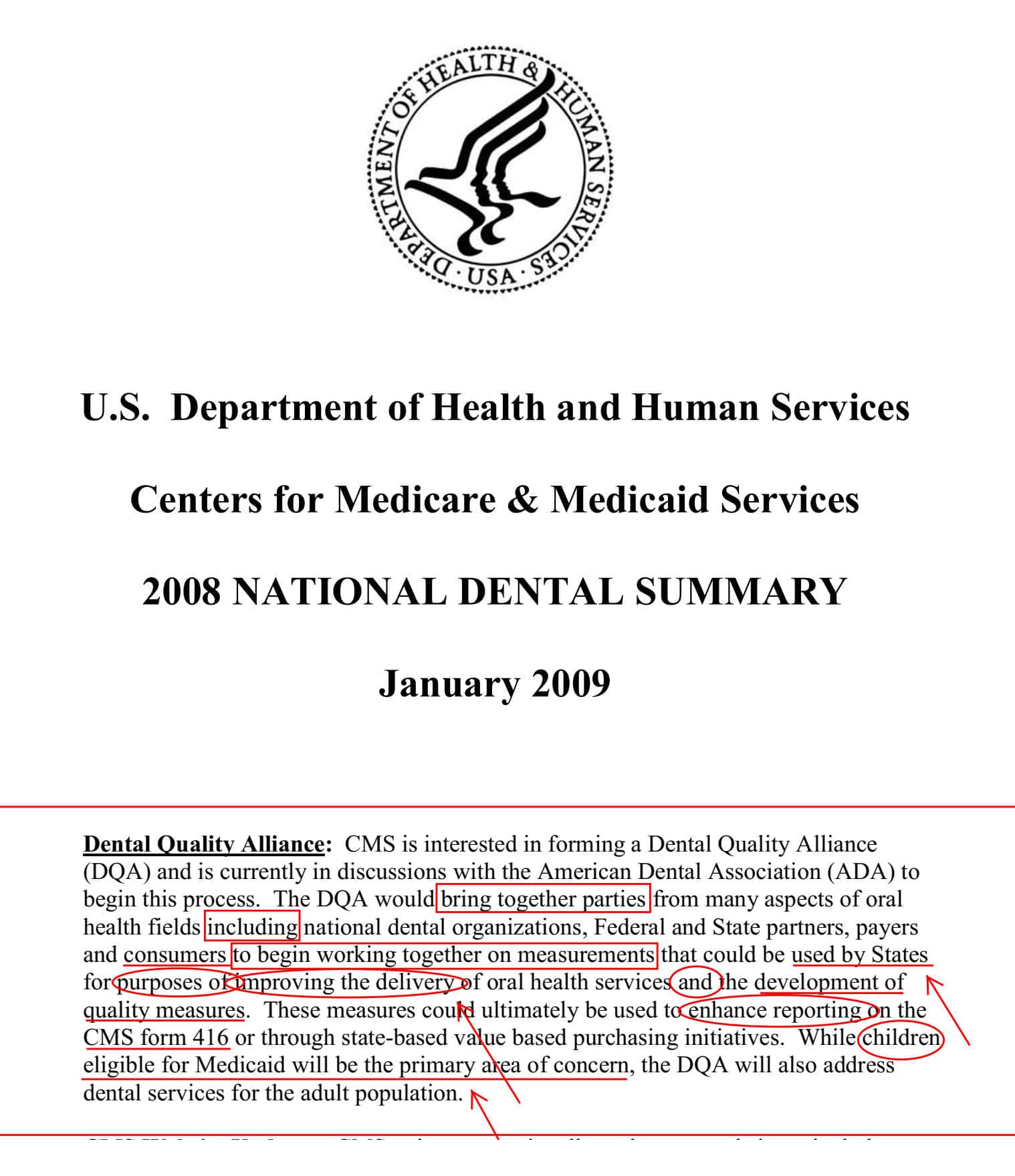
In 2009, the Centers for Medicare & Medicaid Services (CMS) asked the ADA to form a “Dental Quality Alliance” (DQA) – that would bring together various oral health stakeholders (including national dental organizations, federal and state partners, insurance companies, and patients).
The DQA’s intent by CMS was specific:
“work together on measurements that could be used by States for the purposes of improving the delivery of oral health services and the development of quality measures” to be primarily focused on “….children eligible for Medicaid.”
Essentially, ADA’s alliance was supposed to ally with insurers and other stakeholders to influence Children’s Medicaid (not ally to influence all of dentistry).
But this is not what the DQA has been doing since 2009 – far from it.
The DQA’s current mission omits most of these limited directives, and now has an unlimited agenda captured in this published mission:
“The mission of the DQA is to advance performance measurement as a means to improve oral health care, and safety through a consensus-building process.”
The words State, Medicaid, and Children are conspicuously absent from the current broader mission – which means that insurers are no longer invited into the ADA to just give Medicaid advice (which does not directly affect insurer profits).
When asked why the mission changed, this author was informed that DQA members “voted to change the mission.”
Interestingly, insurers buy the right to vote at DQA (detailed below). So DQA insurers paid to vote and adopt a mission that allows them to influence national oral health policy (which directly affects their own profits) – under the honorable banner of the “ADA.”
HOW INSURERS BECOME VOTING MEMBERS OF DQA
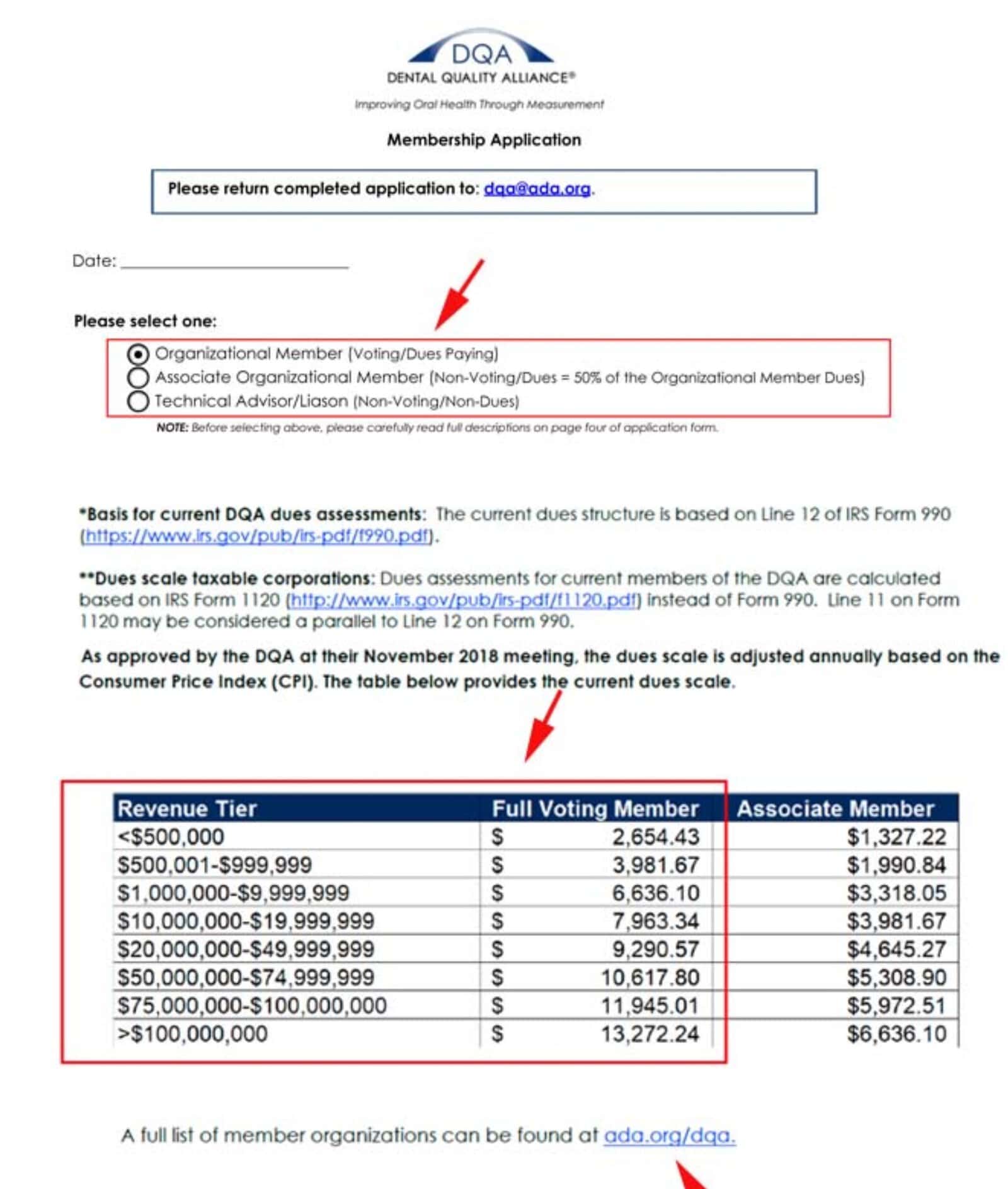
An organization can be a “Full Voting Member” based on a revenue scale: Full voting membership costs from $2,654.43 annually (for revenues under $500,000) to $13,272.24 annually (for revenues over $100 Million).
Organizational members include CareQuest, Delta Dental, DentaQuest, National Association of Dental Plans, and Managed Care of North America Dental.
The current chairman of the DQA is Dr. Linda Vidone, Vice President of Clinical Management for Delta Dental of Massachusetts.
DQA IS PUSHING FOR VALUE-BASED CARE
The DQA is a platform that encourages/ influences policy standards and creates performance measures and strategies to achieve those standards.
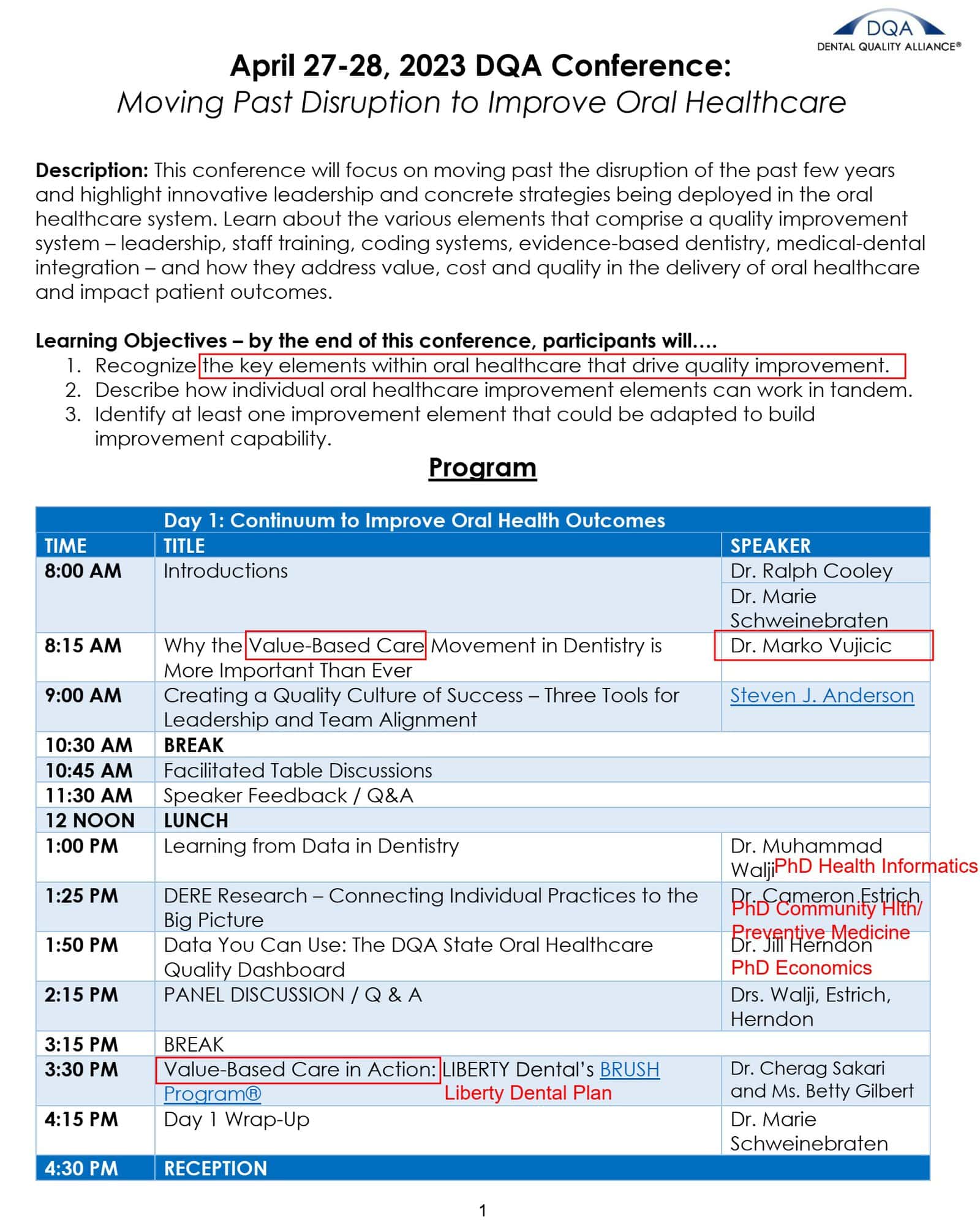
At the April 2023 DQA Conference, most of the presenters were insurers and economists.
Value-Based-Care presentations included:
Cherag Sakari and Betty Gilbert (Liberty Dental Plan) – “Value-Based Care in Action: Liberty Dental’s BRUSH Program.”
Marko Vujicic (a controversial ADA economist discussed later in this article) – “Why the Value-Based Care Movement in Dentistry is More Important Than Ever.”
Mike Adelberg (Director, National Association of Dental Plans – NADP) – “Constructing Value Based Dental Care Brick by Brick.”
DIAGNOSTIC CODING IS A “BUILDING BLOCK” FOR VALUE BASED CARE
Mike Adelberg’s “Constructing Value Based Care….’Brick by Brick’ ” led to another NADP presentation on the same day – this time referring to “Building Blocks:”
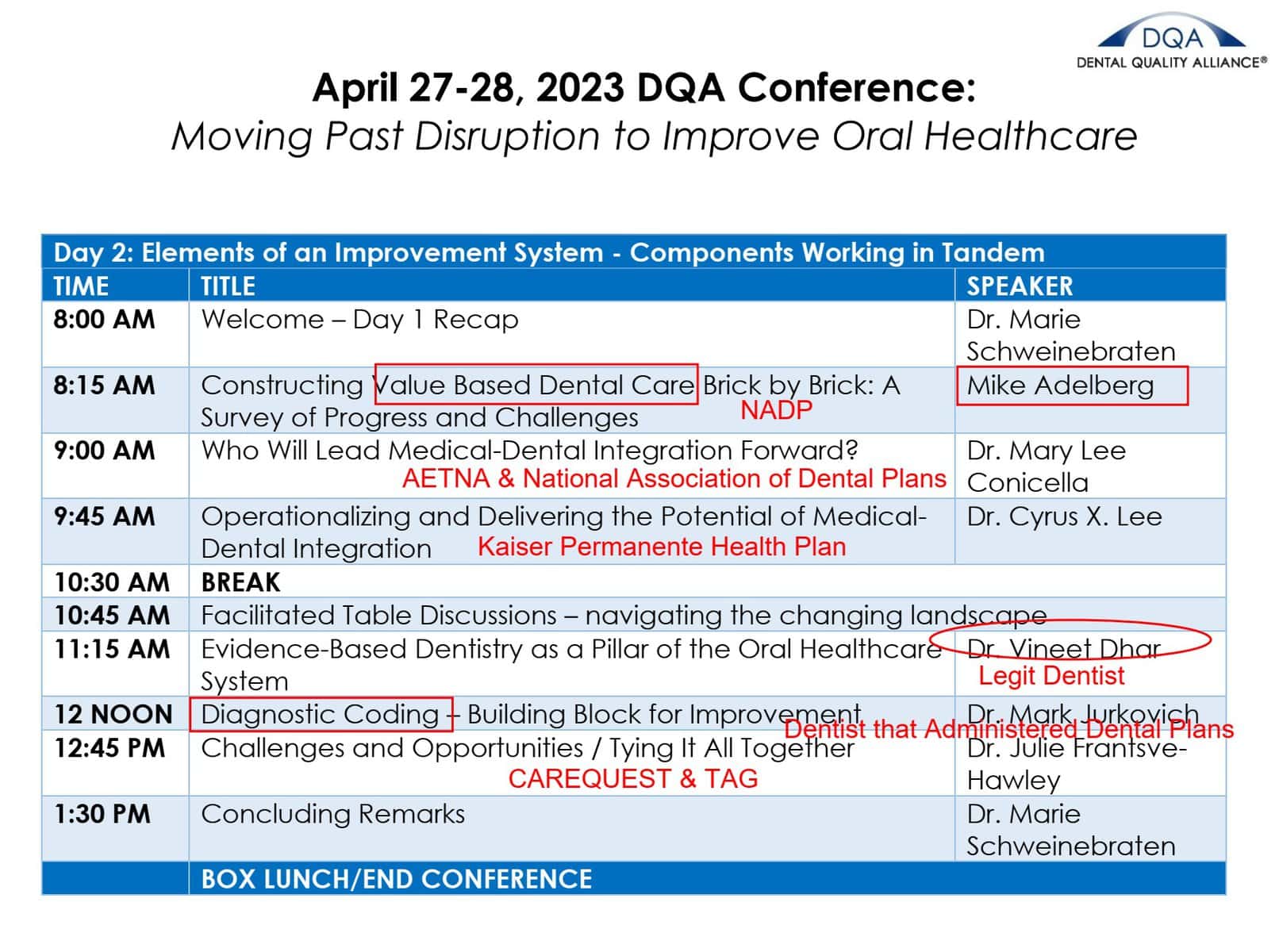
Mark Jurkovich (National Association of Dental Plans – NADP) – “Diagnostic Coding – Building Block for Improvement”
If you are unfamiliar with “Diagnostic Coding” in dentistry, it is because diagnostic codes do not currently exist in dentistry. But insurers want them, and not for the epidemiological data value – but because diagnostic (treatment failure) codes are the missing “building block” to empowering Value Based Care in dentistry.
Diagnostic (treatment failure) coding will lead to another building block – “dentist ratings” based on the diagnostic (failure) codes, as described below.
Diagnostic codes identify “why the procedure was done,” such as recurrent decay, leaky crowns, and other diagnosed treatment failures. These failure codes will retrospectively rate dentist performance (a key requirement of value-based care) – without attributing responsibility to the patient.
Essentially, Diagnostic Coding will be weaponized against dentists, and this will harm patients.
DIAGNOSTIC FAILURE CODING & DENTIST FAILURE RATINGS CAUSE HARM
The combination of Diagnostic Coding and Dentist Failure Ratings will create “gain of function” (using virology language) for the Value Based Care model, which is itself designed to defer treatment.
Dentists will no longer want to immediately treat their failed procedures on their patients. They will instead want to defer treatment, because the failure code they must use will be used against them the sooner it is used. By deferring care, dentists ratings improve (on insurer websites) – patient neglect is incentivized, and insurers pay less for care.
Additionally, Dentists will not want to do much of any treatment under a VBC (Capitation) model, since they are paid a standard monthly fee per capita – patient neglect is incentivized, and insurers pay less for care.
ADA POLICIES AND DQA SUBVERSION
The ADA has a policy against Capitation plans (see previous article) – The DQA directly subverts the policy as described above.
The ADA also has a policy against Dentist Performance Ratings (by insurers) – The DQA indirectly subverts this, by pursuing Diagnostic Coding (which itself empowers Dentist Performance Ratings).
The ADA does not yet have a policy against Diagnostic Coding – which the ADA should quickly create and adopt, in order to protect against Dentist Performance Ratings and VBC.
HPI NOT ALIGNED TO ADA POLICY EITHER – MARKO VUJICIC
The DQA is not alone in subverting ADA policies under ADA’s nose.
Marko Vujicic, leader of the ADA’s Health Policy Institute (HPI) and frequent speaker at the DQA, wrote a June 2023 editorial (shortly after the April 2023 DQA Conference) that encourages dentists to adopt value-based care.
Vujicic wrote “The VBC movement is disruptive, especially to providers. It is not what medical and dental schools have been training students to do.” “If you are a provider reading this and thinking this is a terrible idea, we need to stop this, I can’t control people’s health, or feeling really uncomfortable or angry, you are not alone,” wrote Vujicic.
Vujicic then advises dentists to “Embrace it – accept value-based care as the future model for dentistry” and states “Value-based care requires detailed diagnosis data.” He is pointing to Diagnostic Coding (a building block previously discussed in this article).
Nowhere in the paper is the ADA’s current policy against capitation mentioned. Nowhere in the paper does he refer to the detrimental history of Capitation plans on patients.
Vujicic ends with “VBC is an approach that prioritizes patient’s needs and preferences, aims to achieve optimal oral and overall health outcomes…..This is the future. Let us bring it a step closer.”
After significant backlash from dentists and ADA leadership, Marko wrote an apology for the article. ADA dentists indicated they were not satisfied, believing that a forced apology does not change Vujicic’s desire to subvert ADA policy that protects patients.
For this and similar reasons, many ADA members believe Marko Vujicic is allied to profiteering insurers. Many members have demanded removal from of Vujicic from the ADA – yet he remains and is a favored speaker at the influential DQA.
DQA MEMBERSHIP APPLICATION DENIED FOR AADIQ
Our group, the American Alliance for Dental Insurance Quality (AADIQ), applied to be an organizational member of DQA. We are well known in dental advocacy – having successfully installed the Massachusetts Question 2 law (heralded as the most important dental legislation in the history of the country).
As our name indicates, we work on dental insurance quality, collaboratively – which aligns to the original CMS mission for DQA. And we certainly are in the same space as dental insurers (who we monitor). So if dental insurers pervade the DQA, shouldn’t their monitor (AADIQ) be there?
Yet Dr. Mouhab Rizkallah (President of AADIQ) received a denial letter from DQA that stated:
“After discussion…..in connection with the AADIQ’s ability to support the work of the DQA and whether the AADIQ stated mission is aligned with clinical quality/ performance measure development, the DQA voted not to accept the AADIQ as a member.
Essentially, they feel AADIQ would not support the current work of DQA – they are right.
If “support” is the membership standard, the ADA’s DQA should remove the ADA as well – since ADA policy itself opposes DQA initiatives.
But of course, the DQA would never remove the ADA. It is better to hijack the ADA banner and use it against ADA policy – for as long as the ADA allows it.
Taken together, the DQA has become a rogue group inside the ADA – the foxes literally bought control of the ADA hen house, where they subvert ADA policy.
CONCLUSION
The ADA is the most powerful dental organization in the country, and it was for this reason that CMS relied on the ADA to create a Dental Quality Alliance – to guide states in improving oral health delivery for children on Medicaid.
Instead, the DQA has been an ADA platform for insurance companies to propagate their profit-seeking interests “brick by brick,” by advancing Diagnostic (failure) Codes that will enable Dentist Ratings (by insurers) to give life to Capitation plans (relabeled as Value-Based Care).
This article was meant to provide insight and encourage the ADA to stop allowing the purchase of DQA voting rights (insurers should only have the right to provide comment—not vote—on oral health policy).
It is time for ADA members to take note of the DQA’s activities, and demand that ADA officers act to return the DQA to its original CMS purpose, focused only on Medicaid – with emphasis on Child-Medicaid in every state.
